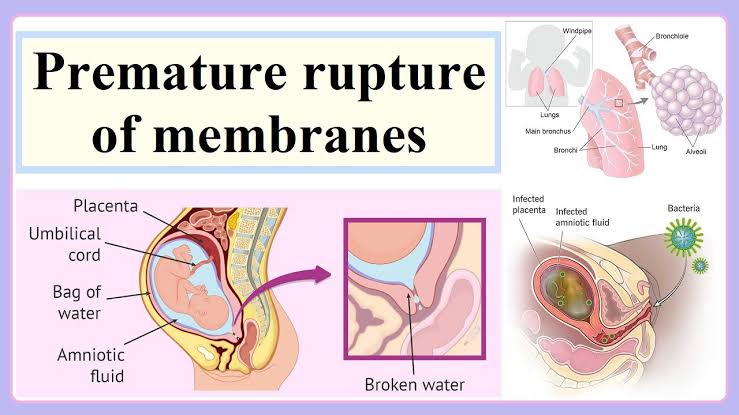
গর্ভকালীন সময়ে পানিভাঙ্গা(Leaking membrane) !!
Mediverse Blog
Catagories:
GYNAECOLOGY
Writer: Dr. Tania Hafiz
2003-2004
গর্ভকালীন সময়ে পানিভাঙ্গাঃ এই সমস্যা নিয়ে রোগী কিন্তুু দুই ধরনের history দিয়ে থাকেন।
১।। হঠাৎ করে ঝপঝপ করে পানিভাঙ্গা
২।। চুইয়ে চুইয়ে, অল্প অল্প পানিভাঙ্গা
এই পানিভাঙা বিভিন্ন কারনে হয়ে থাকে, হতে পারে রোগী লেবারে যাচ্ছে অথবা অন্যকোনো কারন। আমরা যদি রোগীর মধ্যে লেবারের লক্ষনগুলো দেখি তখন একরকমের চিকিৎসা, আর যদি সেই ধরনের লক্ষন না দেখি তাহলে আরেক রকমের চিকিৎসা ও উপদেশ।
আজকে এই বিষয় নিয়েই আলোচনা।
আসুন জানি……….
Examination :
A> At 1st to confirm is it amniotic fluid/Urine/leucorrhoea?
=> So how to understand…
Use a sanitary pad for 30 mins and lay down the patient
When the check pad: if yellowish colour and urinary smell➡ it’s urine
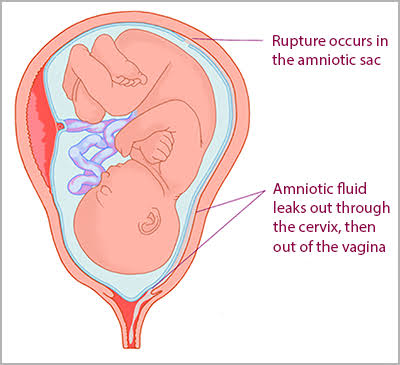
When the pad soaked clear, odourless➡ it’s Amniotic fluid. When patient standing then gash of warm water/leaking al time fluid (steady flow).
Sometimes a bit of cramping and discomfort.
(Note📝: if there is a greenish to brownish tint, contact doctor immediately as it could be a sign baby had a bowel movement in utero)
When sticky/(Curd like), thick something found on pad➡ It’s leucorrhoea.
B> FM, FHS checking
C> Odema
D> To check all vital signs
E> Do Urine, USG
History Taking/ Cause/ Risk factors :
👉Any journey
👉Any heavy or hard work
👉Any intercourse last day
👉Any falling, accident
👉Any heavy weight lifting
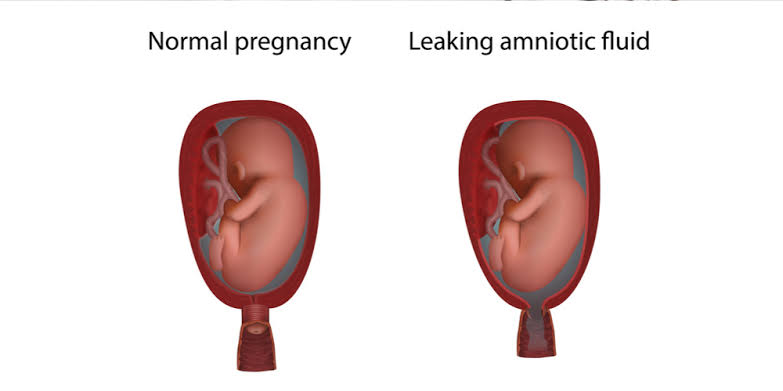
👉Check ultra report excess fluid (polyhydramnions)
👉Any previous disease/ untreated infection
👉Any H/O BV, STD
👉Any Smoking history
👉Had a previous early membrane rupture
👉Have Placenta Abruption
👉Are Carring twin or multiple pregnancies
Complications/ What happen when AF leaks :
1. Many women go into labor in about 24hrs of amniotic membrane rupture or leaking.
2. Infection both mother and baby
3. Placenta separate from uterus
4. Umbilical cord problem
5. Premature Birth
6. Sometime need C/S delivery
Treatment and Advice :
1. At 1st Advice: Admission in hospital for observation and better Management:
(নোট📝ঃরোগী আপনাকে বলবেন যে “আমিতো বাসায় রেস্টেই থাকবো, কোনো কাজ করবোনা, আপনি আমাকে মেডিসিন দিন”। কিন্তুু বেশিরভাগ ক্ষেত্রেই দেখা যায় যে রোগী কিছু না কিছু কাজ করবেই তখন সেই ভারী কাজ করার ফলে তার আরো পানি ভাঙতে থাকবে এবং এরফলে বাচ্চা র যেকোনো ক্ষতি হতে পারে, আর হাসপাতালে অবজারভেশনে থাকলে সেই সুযোগ হচ্ছে না, এমনকি রোগীর vital sign monitoring, foetal movement + heart beat টাইম টু টাইম মনিটরিং করা হয়। বাচ্চার অবস্থা খারাপের দিকে গেলে সাথে সাথে সিদ্ধান্তও নেয়া যাবে। সুতরাং এগুলো রোগীকে বুঝিয়ে বলতে হবে। এবং অবশ্যই প্রেসক্রিপশনের প্রথমেই ” Advice: Admission in Hospital” কথাটা লিখে রাখতে হবে আমাদের নিজেদের সেফটির জন্য।
2. Complete bed rest
3. Avoid constipation, cough.
4. Namaz on lying position
5. Always observe baby’s movement 10-12 times in 12 hours.(if patient can’t count just pad & pen given to observe )
6. TT schedule maintain
7. Antibiotic given
8. Injection Dexamethasone At before or at 34wks for maturity of fetal lung
9. If Fetal movement less then O2 inhalation
10. Continue all prescribed drug like iron, folic acid, Calcium properly.
11. Do all pregnancy profile tests. Specially F/up Usg for amniotic fluid.
12. Personal hyigene maintain
13. Avoid stress, heavy work/heavy wt lifting, intercourse etc etc
14. Regular Antenatal checkup
Note📝📝: Always concern about pregnant patient. Bcz they live with a stress/tension. So if any problem arise like PROM/bleeding/ LAP/ less fetal movement then they become scared which hampered her baby.
So as General practitioner we always take care our patient properly.
Edited by : Nahid Hassan
Share this blog to social media:
Tags:
Leaking membrane
Prom
Tania Hafiz
Suggested post
No post related to the current post. Please click on 'view more' to see more posts